Table of Contents
Introduction of Gastroesophageal reflux disease (GERD)
Gastroesophageal reflux disease (GERD) is a common gastrointestinal condition in ambulatory settings. In the USA, GERD remains the commonest cause of outpatient hospital visits and economic burden costs around $15-20 billion per year. Studies from the Asian subcontinent have also reported significant absenteeism, loss of work productivity, and weekly burden of $165.07 per person.’ GERD is not confined to acid-peptic complications and comprises a broad spectrum of conditions with varying symptoms and complications. Patients with GERD require personalized medical care based on the presenting symptom and underlying mechanism of the disease. Recent advances in the diagnostic evaluation of GERD have identified pathological dysfunctions and categorized patients into different subgroups. Treatment of GERD is also evolving from a one-size-fits-all approach centered on empiric acid suppression to phenotype-guided treatment. This chapter will review the definition, clinical spectrum, and natural history of GERD.
Definition of Gastroesophageal reflux disease (GERD)
The symptoms of GERD are driven by the backward flow of gastric content into the esophagus. Gastroesophageal reflux (GERD) is a physiological phenomenon during the early postprandial phase. When the threshold of reflux normality is passed, GER may induce inflammatory changes to the esophageal mucosa and present various symptoms. Despite, multiple studies on GERD in the general population no consensus definition was available till 2006.
In 2006, Montreal Consensus defined GERD as “a condition which develops when the reflux of stomach contents causes troublesome symptoms, impairs quality of life, or leads to mucosal damage and/or complications”? The definition included the term “troublesome” to describe the negative effect of the symptoms on the individual’s quality of life. The consensus included retrosternal burning (heartburn) and regurgitation as the characteristic symptom to define GERD.
Clinical presentations
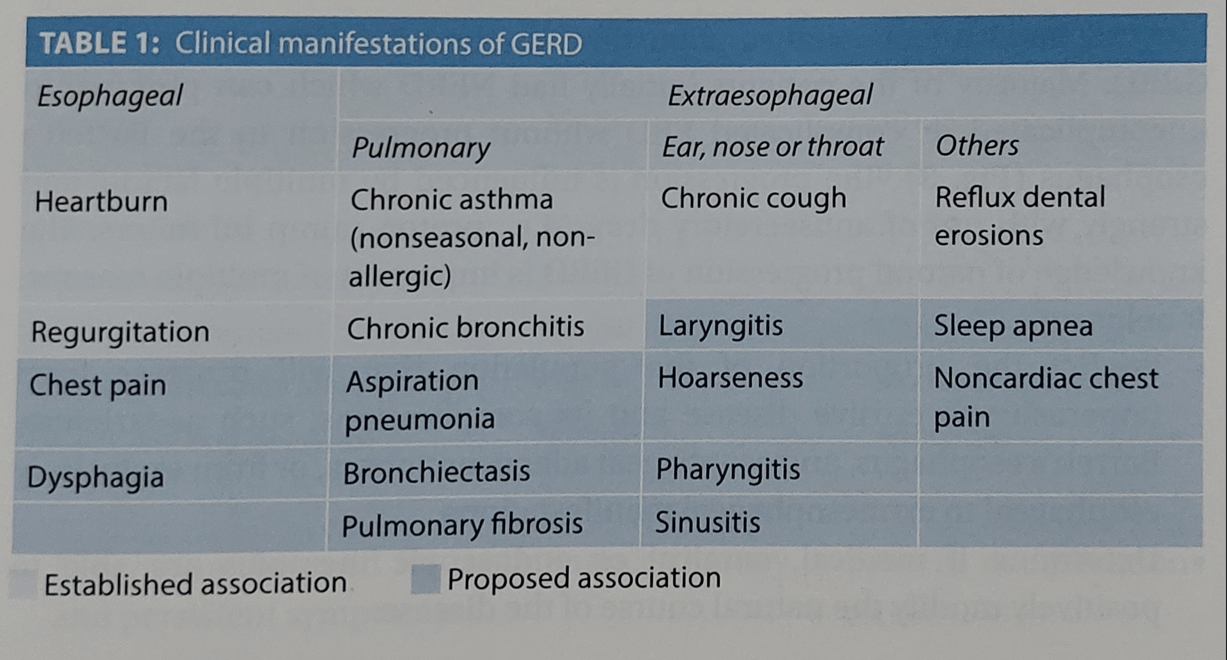
The concept of the GERD clinical spectrum has changed vastly in the last decade. The disease has a natural tendency to progress in the absence of treatment and can present with many faces. GERD encompasses a large clinical spectrum of signs and symptoms. It affects not only the esophagus but also many other organs, including the mouth, lungs, ear, nose, and throat, and can be accompanied with or without esophageal signs (Table 1). Patients of GERD can be categorized into three broad symptom profiles (Figs. 1 and 2):
1. Patients with typical symptoms, e.g., heartburn and regurgitation but without endoscopic evidence of reflux esophagitis, called as non-erosive reflux disease (NERD). It constitutes the majority of patients at diagnosis, up to 70%.
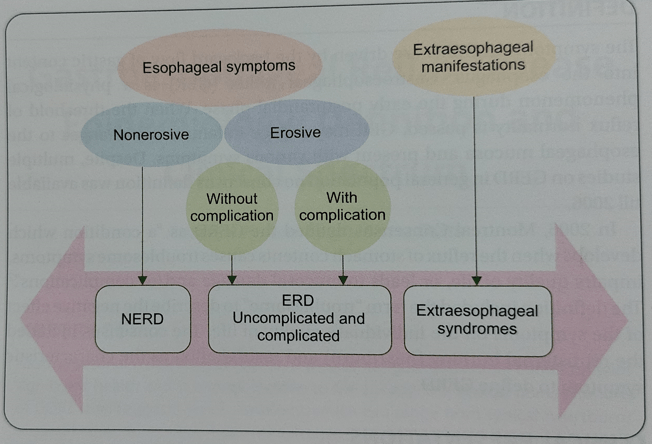
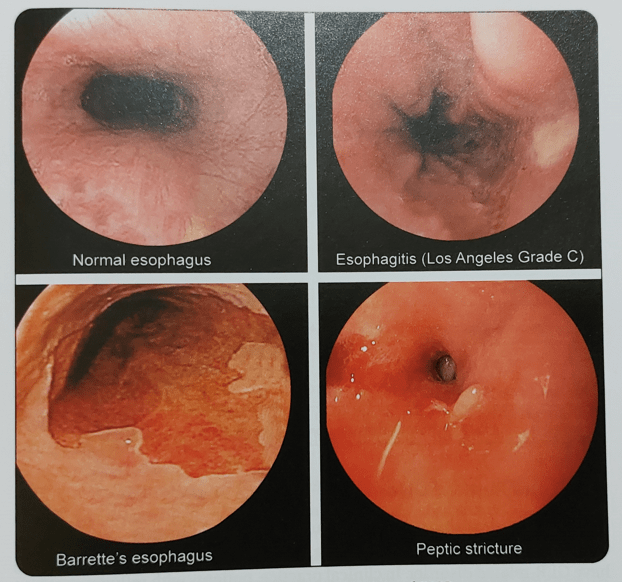
2. Patients with evidence of reflux esophagitis, may further present with or without associated complications, such as peptic esophageal stricture or intestinal metaplasia.
3. Patients with extraesophageal manifestations.
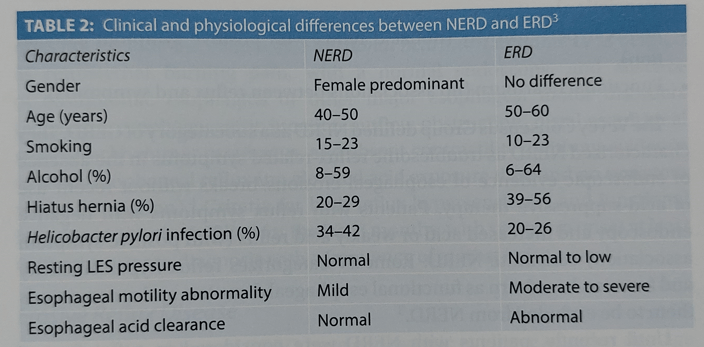
Based on symptoms, it is difficult to classify the patient as NERD or erosive reflux disease (ERD). Several clinical and physiological characteristics can help in differentiating NERD from ERD (Table 2).
The spectrum of GERD and natural history
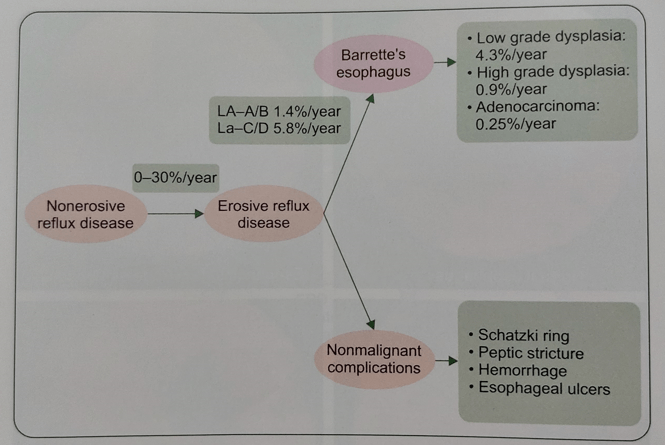
Most of the available studies point towards the progressive nature of the GERD. The majority of the patients initially had NERD which can progress to uncomplicated or complicated ERD without progression to Barrett’s esophagus (Fig. 3). The progression is influenced by multiple factors and strongly with the use of antisecretory drugs, i.e., proton pump inhibitors. The knowledge of the natural progression of GERD is important for multiple reasons.
It helps to:
- Predict the proportion of the population that will progress from non-erosive to erosive disease and its complications, such as stricture, Barrett’s esophagus, and esophageal adenocarcinoma, or from exclusively esophageal to extraesophageal manifestations.
- Determine if medical, surgical or endoscopic therapies are able to positively modify the natural course of the disease.
- Determination of the need for maintenance therapy to prevent complications and persistent symptoms.
NERD and Related Disorders
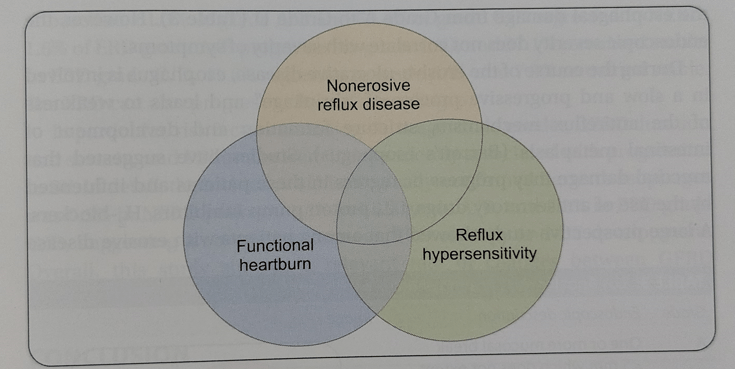
People with heartburn but without erosive esophagitis comprises a heterogeneous group of patients (Fig. 4). Some of these patients may not have GER-related disorder. In clinical practice, patients with reflux symptoms and negative endoscopic findings can be categorized as:
- NERD (increased acid or weak acid reflux with positive symptom association).
- Reflux hypersensitivity (nonacid reflux with positive symptom association).
- Functional heartburn (no associations between reflux and symptoms).
The Vevey Consensus Group defined NERD as a subcategory of GERD. They characterized NERD as troublesome reflux-related symptoms in the absence of endoscopic evidence of esophageal erosions/breaks without the recent use of acid-suppressive therapy. Patients with reflux symptoms with negative endoscopy and increased acid or weakly acid reflux (with positive symptom association) constitute NERD. Rome IV categorizes reflux hypersensitivity and function heartburn as functional esophageal disorders and recommends they be excluded from NERD.
Until recently, patients with NERD were considered to suffer from a milder disease requiring less intensive treatment and a better long-term prognosis. However, this concept is challenged by similar impairment of disease-related quality of life (HRQOL) in non-erosive and erosive reflux disease. The symptom response to PPI is similar or even worse in patients with NERD compared to erosive reflux disease. Studies evaluating the natural history of GERD suggest that patients with NERD progress from non- erosive form to erosive GERD.
Rome IV defines reflux hypersensitivity as retrosternal symptoms, i.e., heartburn or chest pain with a normal endoscopy. The definition needs to exclude organic esophageal disorder including eosinophilic esophagitis or major esophageal motor disorders (achalasia, esophagogastric junction outflow obstruction, distal esophageal spasm, Jackhammer esophagus, and absent contractility) as the etiology of symptoms. The symptoms are triggered by reflux events even with normal acid exposure on pH or pH- impedance monitoring. Importantly, response to antisecretory therapy does not exclude the diagnosis. Functional heartburn in Rome IV is defined as retrosternal burning pain, with normal endoscopy, and absence of eosinophilic esophagitis or other major esophageal motor disorders (achalasia, esophagogastric junction outflow obstruction, distal esophageal spasm, Jackhammer esophagus, and absent contractility), without evidence of gastroesophageal reflux (no elevated acid exposure time and no symptom reflux association). Criteria for both reflux hypersensitivity and functional heartburn must be fulfilled for the last 3 months, with symptom onset at least 6 months prior to diagnosis with a frequency of at least twice a week.
Products to keep your gastrointestinal tract Healthy:
Erosive Reflux Disease
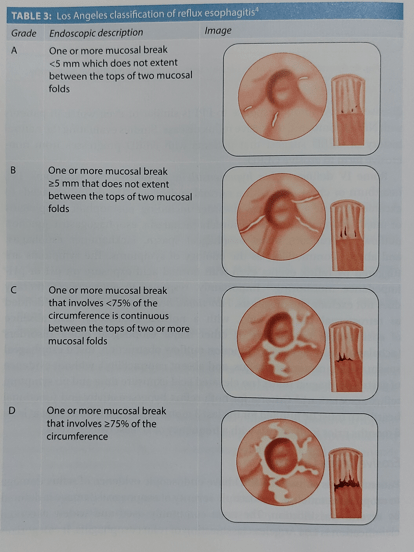
Patients in this subset of GERD have endoscopic evidence of reflux damage to the esophageal mucosa. The endoscopic severity of esophageal damage is defined by several classifications. The most commonly used and widely accepted classification is the Los Angeles classification of reflux esophagitis. It categorizes the esophageal damage from Grade A to Grade D (Table 3). However, the endoscopic severity does not correlate with the severity of symptoms.
During the course of the erosive-ulcerative disease, the esophagus is involved in a slow and progressive process of “shrinkage” and leads to weakness of the antireflux mechanism, stricture formation, and development of intestinal metaplasia (Barrett’s esophagus). Studies have suggested that mucosal damage may progress or regress in these patients and be influenced by the use of antisecretory drugs, i.e., proton pump inhibitors, and H-blockers. A large prospective study showed that among patients with erosive disease at baseline, 61.3% of grade A/B and 50.4% of grade C/D regressed to NERD, 1.6% of ERD grade A/B progressed to grade C/D, and 37.1% remained stable. In ERD grade C/D, 41.8% regressed to grade A/B, and 7.8% remained stable. The ERD can also progress to Barrett’s esophagus.
In particular, risk factors including older age, male gender, GERD duration and severity, and PPI intake were independently associated with progression to BE. In detail, the incidence of histologically-confirmed Barrett’s esophagus was 0.5% in NERD patients, 1.4% in ERD grade A/B, and 5.8% in ERD grade C/D, suggesting a correlation between ERD severity and BE development. Overall, this study showed a relevant rate of changes between GERD categories, thus supporting the spectrum disease hypothesis.
Also, read: Soft gelatin capsule
Conclusion
Gastroesophageal reflux disease (GERD) is a common gastrointestinal condition characterized by heartburn and regurgitation with a significant effect on quality of life. GERD includes a broad spectrum of conditions that are not confined to acid-peptic complications only and the spectrum extends from NERD to Barrett’s esophagus and esophageal adenocarcinoma. Available studies suggest the benign nature of NERD and mild esophagitis which tend to resolve with time or remain as such. A proportion of patients can progress from non-erosive to erosive esophagitis (0 to 30%), from mild to severe ERD (10 to 22 %), and from ERD to Barrett’s esophagus (1 to 13%).