The tampon is made of highly absorbent polyacrylate, which concentrated water, magnesium, iron, and oxygen and enhanced the growth of Staphylococcus or Streptococcus, which are part of the normal vaginal flora. Increased magnesium concentrations triggered the production of TSST-1 or SPE-A. During tampon removal, the vaginal wall is often torn allowing TSST-1 and SPE-A direct access to the bloodstream. In the use of following tampon of toxic shock syndrome and significant mortality occurred.

Table of Contents
Toxic shock syndrome
Fever, vomiting, diarrhea, hypovolemic shock, and multi-organ failure are all symptoms of Staphylococcal toxic shock syndrome, which develops quickly (within 8–12 hours). In most cases, death occurs within 24 to 36 hours. T cells stimulated by superantigen release a lot of cytokines including TNF- and IL-1. These cytokines, in combination with TSST-1, increase vascular permeability, resulting in fluid leaking into tissue and acute diarrhea. Less blood is available for the heart to pump as a result of electrolyte and fluid loss. Hypovolemic shock is caused by a substantial decrease in cardiac output. Reduced tissue perfusion harms the kidneys, heart, and lungs over time. Death is the outcome of cardiac failure.
Different toxic shock symptoms are elicited by streptococcal superantigens and pyogenic toxins. Adult respiratory distress syndrome, shock, and renal failure are all symptoms of sTSS. Despite intensive medical therapy, between 30 and 70 percent of patients die.
Treatment
The goal of pharmacotherapy is to eradicate the infective agent. Careful consideration must be given to the identification of the etiologic agent and the antibiotic resistance patterns. Antibiotics used in the treatment of toxic shock are shown in the Table given below.
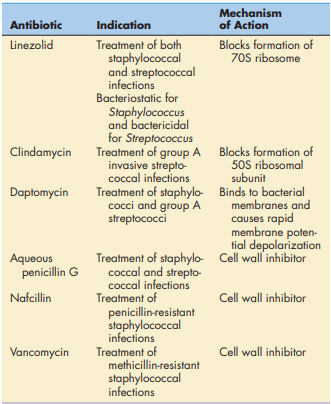
of Toxic Shock Syndrome
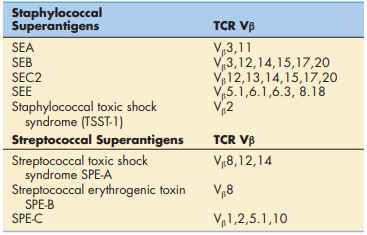
Vβ Isoforms and Superantigen-Induced Clinical Symptoms
Only a small number of people are at risk of developing superantigen-induced clinical symptoms. The presence of genetically determined TCR V isoforms increases the risk. There are fifty-two potential V genes. Only people who have a V2 TCR are at risk of getting sTSS . Individuals who express V8, 12, or 14 TCRs are also at a higher risk of streptococcal toxic shock (showing in the table given below).
Superantigens
Make sure to check our amazing article: Interactions Between T Cells and Antig