Table of Contents
DiGeorge Syndrome
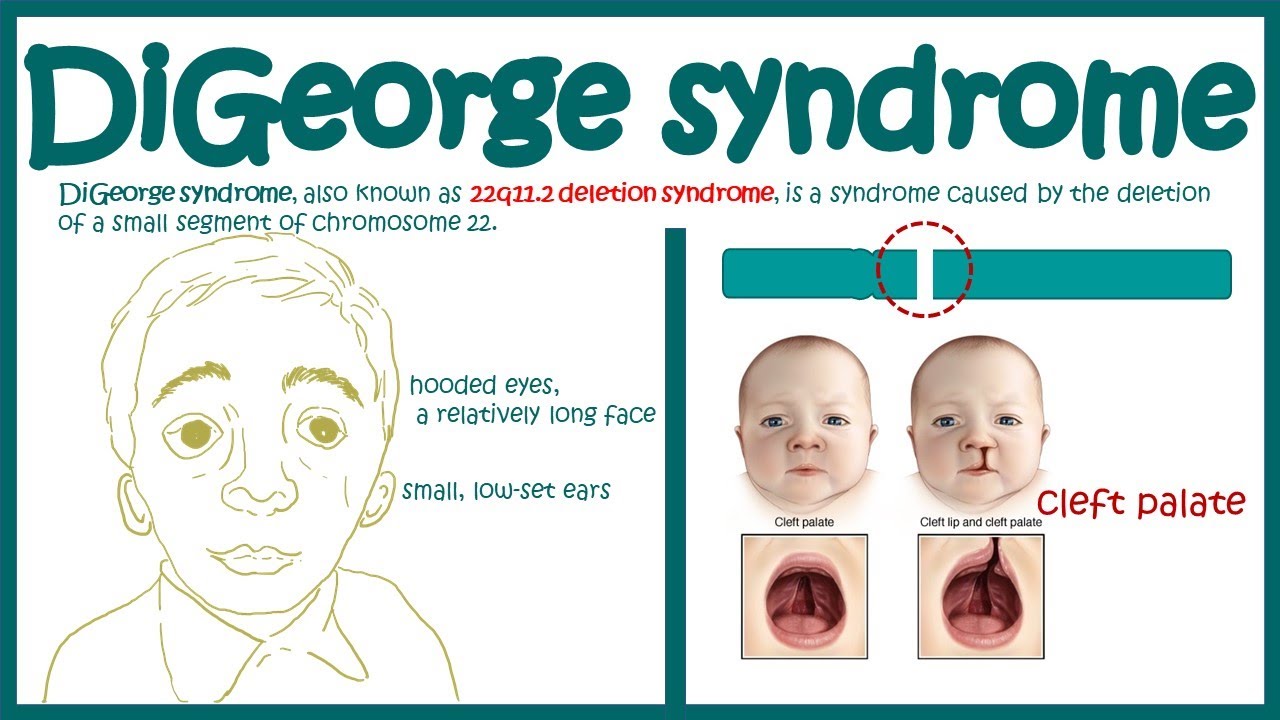
DiGeorge syndrome is caused by the abnormal migration of cells
to select tissues during development. The major defect is a
30-gene deletion on chromosome 22 at position 22q11.2. This
deletion prevents the development of the third and fourth pharyngeal
pouches during the twelfth week of gestation. Major
organs affected by the defect are the thymus, the parathyroid,
and the heart. In addition, facial abnormalities, including
underdeveloped chins, droopy eyelids, and upper ears that are
rotated backward, occur. Children with this syndrome have a
nonfunctioning, rudimentary thymus, and lack mature T cells
in the circulation and in secondary lymphoid tissue. Because
the underdeveloped parathyroid cannot control calcium levels,
muscular tetany and seizures are common. Most of the
deaths are associated with infection or cardiac problems.
Nezelof Syndrome
Nezelof syndrome is a very rare disease that has affected less
than 200,000 children in the United States. Affected children
have a rudimentary thymus, but their parathyroid function is
normal.
Although classified as a primary T cell deficiency, Nezelof
syndrome has associated defects in B cell development and
maturation. Some classifications place the syndrome in the
severe combined immunodeficiency category. Evidence indicates
that children exhibiting only a T cell deficiency have a
purine nucleoside phosphorylase (PNP) deficiency in the
purine salvage pathway. Metabolites are toxic to developing
T cells. In some instances, adenosine deaminase (ADA)
enzymes also are nonfunctional. Toxic metabolites that are
generated as a consequence of the ADA deficiency block the
development of T cells, B cells, and NK cells.
Leukocyte Adhesion Deficiency
Defective diapedesis is reflected in two immunodeficiencies
called leukocyte adhesion deficiency (LAD) I and II. LAD I is
an autosomal recessive disease, in which expression of CD18
on macrophages, neutrophils, and lymphocytes fails to occur.
CD18 consists of LFA-1, macrophage-antigen-1 (MAC-1),
and receptors that bind leukocytes to the molecules expressed
on the endothelium of the blood vessel.
LAD II is the result of defective fucose transport and
fucosylation, which are necessary for the synthesis of sialyl-
Lewisx (s-Lex) on PMNs and monocytes. As a consequence,
monocytes and PMNs cannot exit the vasculature in response
to infections or tissue damage. The disease is extremely rare,
with only 200 cases reported in the last 20 years. Unfortunately,
most individuals with this disease die of overwhelming
infections within the first 2 years of life.